After a year of anticipation, we were witness to a highly complex and decentralized COVID-19 vaccination launch that left many frustrated but, eventually, vaccinated. Driven by a large-scale community effort, 162 million residents have secured vaccine appointments and became fully vaccinated, as of July 2021.
As the Delta variant drives infection rates among the unvaccinated and mask mandates being reconsidered, this summer represents a crossroads for our vaccination efforts. At U.S. Digital Response, we helped build a collective and central vaccine appointment system, partnering with federal, state, and local agencies, major vaccine providers (including Walgreens, CVS, and state-sponsored vendors) and community organizations (including Vaccine Spotter and Vaccinate the States) to make finding an appointment more accessible.
This open data platform spans across the 50 states and over 35,000 local jurisdictions, giving us a birds-eye view on how an equitable and efficient vaccine allocation process could truly work — and exactly how we can drive up vaccination rates. The data contained in our system is read-only, anonymized, and does not contain any personally-identifiable information (PII) about residents or employees using the underlying appointment systems.
With 50% of US residents still not fully vaccinated, we’ll be elaborating on 3 key takeaways across the US from this data platform by spotlighting a diverse set of jurisdictions as tangible examples:
- Appointment data reveals on-the-ground supply and demand dynamics.
- There are equity consequences tied to appointment availability and flexibility.
- Higher appointment flexibility, especially more weekend availability, correlates with higher vaccination rates.
Appointment data immediately reveals on-the-ground supply and demand dynamics
Knowing when appointments are available and how they get booked helps us understand how the volume of vaccine supply meets the demand. For example, here are the average number of slots per 1000 people that were available during April 2021 in California, by time of week:
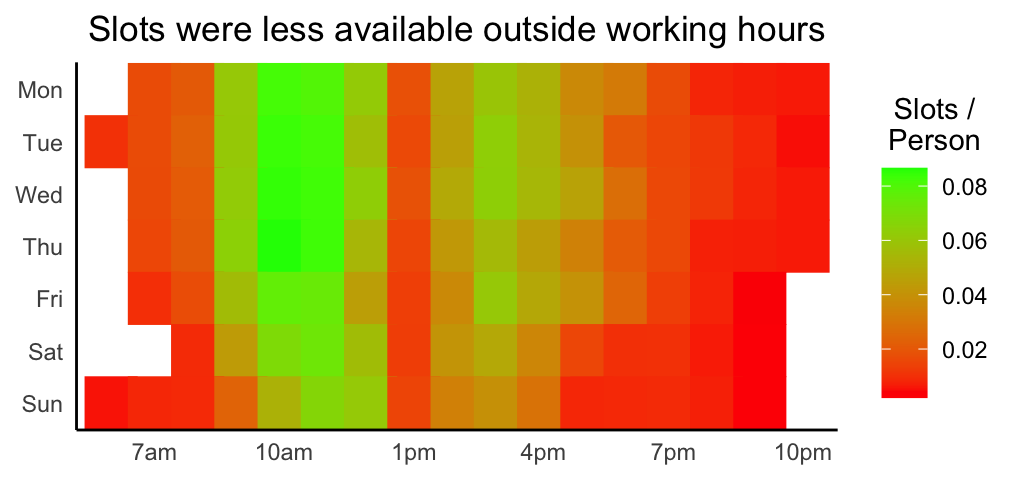
There were fewer slots available outside typical working hours than during the standard work day. Nationally, this trend is even starker: there were 41% fewer weekend slots than work day slots. This is a potential concern since it is hard for a large share of working-age people to get time off from work for medical purposes like getting the vaccine.
Similarly, here is the average number of hours that slots were available for, according to our data:
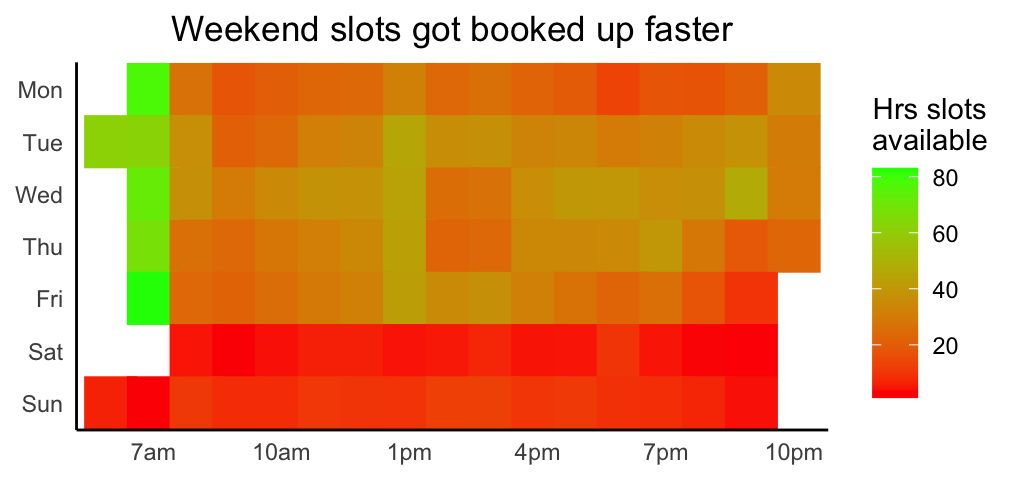
Weekend slots were booked much faster than slots during the week day. The slots that were booked the slowest were before 8 am. Nationally, weekend slots were booked 54% faster than week day slots. This reveals that, compared to the available supply, demand was much higher for weekend slots. When someone has limited availability, and appointments are already scarce, it takes a significant investment to monitor appointment times that fits in with their schedule.
Both of these views indicate that appointments outside of standard working hours were much harder to book. The policy implication is clear: due to the scarcity of appointments outside of working hours, giving people paid time off to get their vaccine may increase their likelihood of being vaccinated, therefore driving overall vaccination rates higher, faster. This work flexibility is particularly critical to reduce barriers for working class residents, especially those who are hourly wage employees.
There are equity consequences tied to appointment availability and flexibility
Another operational angle to vaccine distribution is how equitable it is. We know, for example, that both areas with a higher socioeconomic vulnerability and areas with a larger Black population have seen lower vaccination rates. This increased vaccine hesitancy can be partially attributed to historically-rooted cultural factors, like low-trust toward the medical establishment and limited information access. However, in our data we also see correlations between social vulnerability and appointment access. For example, counties with a higher social vulnerability index (SVI) tended to have fewer appointments available in May 2021. The circles in the plot below represent counties, and their size represents the number of residents in each county.
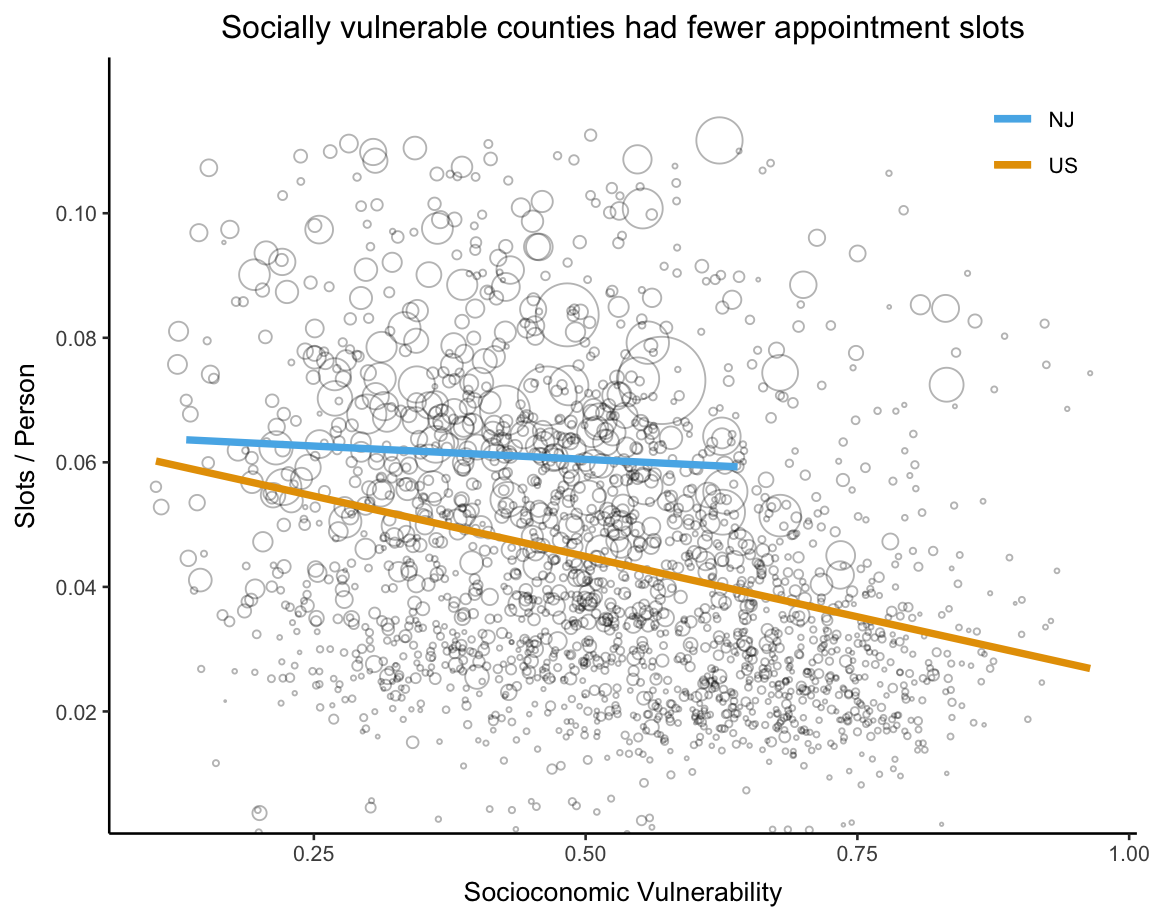
Specifically, the 20% most socially vulnerable counties had almost 60% fewer slots per person and a similar discrepancy exists for weekend slots. Fortunately, this pattern does not hold true everywhere. In New Jersey, our data showed little to no relationship between social vulnerability and vaccine access. Policy decisions matter: this may very well be attributed to the State’s explicit focus on health equity for vulnerable population groups. The relationship between social vulnerability and appointment access is also not always negative. For example, we don’t see a similar relationship between these SVI metrics, and how long appointments are available for.
Higher appointment flexibility correlates with higher vaccination rates
Especially for residents who are on the fence about getting fully vaccinated, the ease of scheduling an appointment affects whether someone is willing to do so. Indeed, according to our analysis, more flexible access to vaccine appointments is correlated with increased vaccination rates. This suggests that increased flexibility in booking appointments could have had a positive effect on vaccination rates. We measured flexibility of access in three ways:
- Number of appointment slots per resident
- Relative prominence of slots during the weekend
- Average number of hours that an appointment was available before being booked
As an illustration, during the month of April 2021, both Dodge County and Chippewa County in Wisconsin had a similar amount of appointments available per person, and they have a similar population and vaccine hesitancy (according to this CDC survey). However, taking into account these controlled factors, Dodge County had 70% more weekend slots than Chippewa–and also had 5% more vaccinations during this time.
This example was cherry-picked, but the pattern remains when we consider all jurisdictions and control for other factors like population size, vaccine hesitancy, and resident demographics. Counties with more slots per person saw higher vaccination rates, but the impact on higher vaccination rates of an extra weekend slot is much stronger than the effect of an extra slot during the week.
A statistical caveat to note: while in our data appointment availability and flexibility are predictive of increased vaccinations, this doesn’t mean that these factors necessarily cause more vaccinations. For example, how long an appointment slot is available for is also an indicator of vaccine demand. The direction of the causation is not obvious: appointment availability may simply be a proxy for demand, and thus vaccinations, rather than a cause.
Moving forward
While a broader challenge is to increase the intent of millions of unvaccinated residents in the US, we hope that this data platform’s insights can pair with community education work, so that minds changed quickly and easily transitions to lives saved.
Beyond this post’s retroactive insights, this vaccine data platform is real-time and flexible: we can support making smart policy and operational decisions with a wide range of data offerings, like systematic reporting and dashboards monitoring critical vaccination supply and demand metrics, cross-geo comparisons, metric threshold alerting, and custom analyses diving deeper.
This data platform is publicly accessible, and the code for this analysis can be found in this GitHub repo here.
U.S. Digital Response is partnering with governments and nonprofits across the country to address needs related to the COVID-19 crisis, including vaccine preparedness and communications. To learn more about USDR’s work, visit our website for a full menu of USDR’s health-focused offerings.
If you are a government or nonprofit seeking assistance with your communications strategies or COVID response efforts, connect with our team by filling out this brief intake form and we’ll get back to you within 24 hours.
